

By Henrylito D. Tacio
James Adlawan (not his real name) is your typical 40 years old. But when he learned that two of his cousins have been diagnosed of colon cancer, he decided to go to the Lanang Premiere Doctors Hospital in Davao City for a screening colonoscopy. “It’s better safe than sorry,” he said.
Dr. Paolo O. Dillera, the gastroenterologist who did the screening, saw a large, elevated, sessile polyp with a regular tubular surface pattern. He thought of it as either an adenoma or low-grade intramucosal neoplasia.
“If not detected and removed early, it has a high chance of developing to cancer,” Dr. Dillera said. “Luckily for this patient, he thought of prevention rather than cure.”
The good news is: that deaths caused by colon cancer have been dropping steadily over the last two decades, according to St. Luke’s Medical Center’s Dr. Alexandra Laya-Zinampan, whose specialties are gastroenterology and internal medicine.
“This can be attributed to the fact that colon cancer screening advocated at 50 years of age with colonoscopy not only detects the existence of pre-cancerous polyps,” she explained. “It also allows the removal of any polyps that may develop into cancer later on in life.”
Now, the bad news: the incidence of colon cancer among adults under the age of 50 have been increasing steadily. “This may be because younger patients do not notice any symptoms to prompt testing before the recommended time,” Dr. Laya-Zinampan said. “Treatment can be delayed and the risk of colon cancer causing death will again increase.”
In a news conference, Dr. Frederick Dy of the Philippine Society of Gastroenterology (PSG) was quoted as saying by Philippine Star: “Over the past year, we thought, in the gastrointestinal tract, the liver is supposed to be the number one cancer in the Philippines. But right now, it has been overtaken by colorectal cancer.”
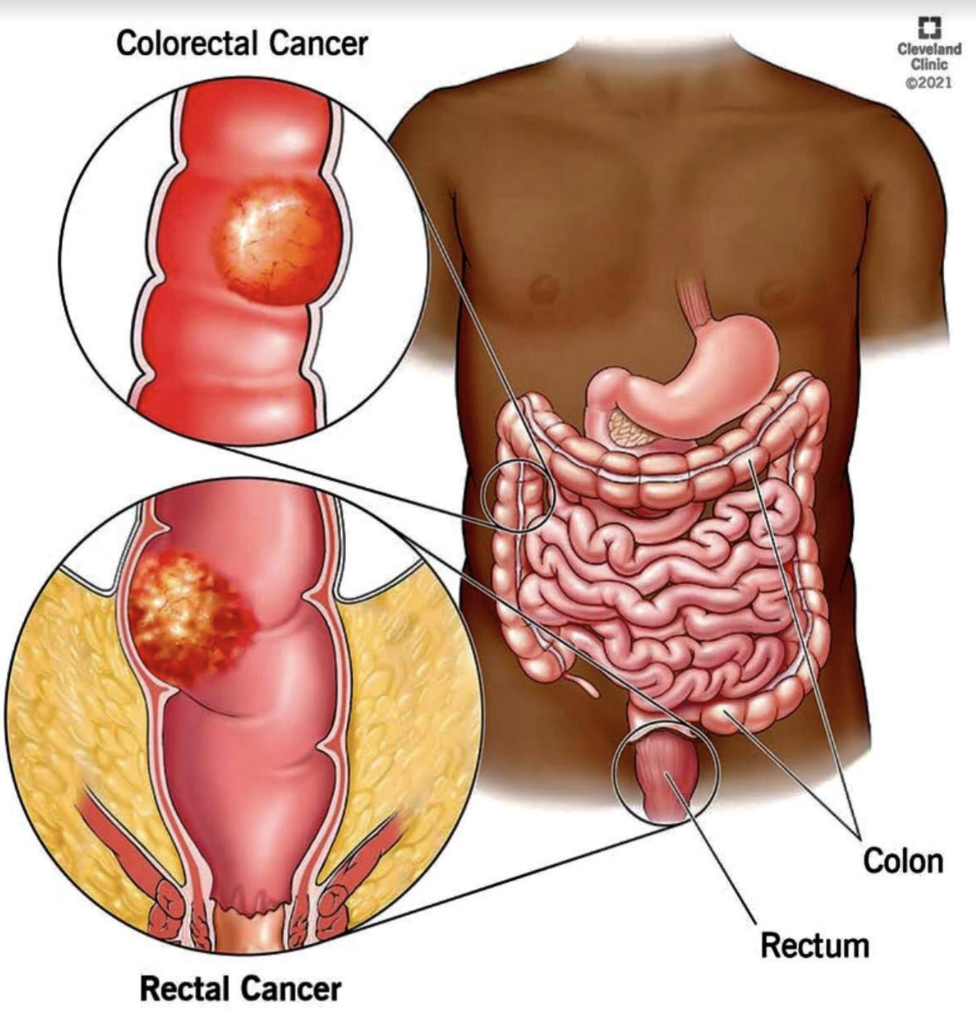
Colon cancer is the more common name, but this type of cancer also includes rectal, thus, it is called colorectal (CRC). Both are often grouped together because they have many features in common. For instance, both cancers begin in the digestive system, also called the gastrointestinal system. The digestive system processes food for energy, and the last part of it absorbs fluid to form solid waste (stool) that then passes from the body.
“After food is chewed and swallowed,” states the American Cancer Society (ACS), “it travels to the stomach. There it is partly broken down and sent to the small intestine.” The small intestine is the longest part of the digestive system – about 20 feet.
“The small intestine also breaks down the food and absorbs most of the nutrients. It leads to the large intestine (also called the large bowel or colon),” explains the ACS. “The colon absorbs water and nutrients from the food and also serves as a storage place for waste matter. The waste matter moves from the colon into the rectum, the last 6 inches of the digestive system. From there, the waste passes out of the body.”
Cancer that starts in any of these areas may cause different symptoms. Another common thing between colon cancer and rectal cancer is that, depending on where they start, the cancers develop slowly over many years.
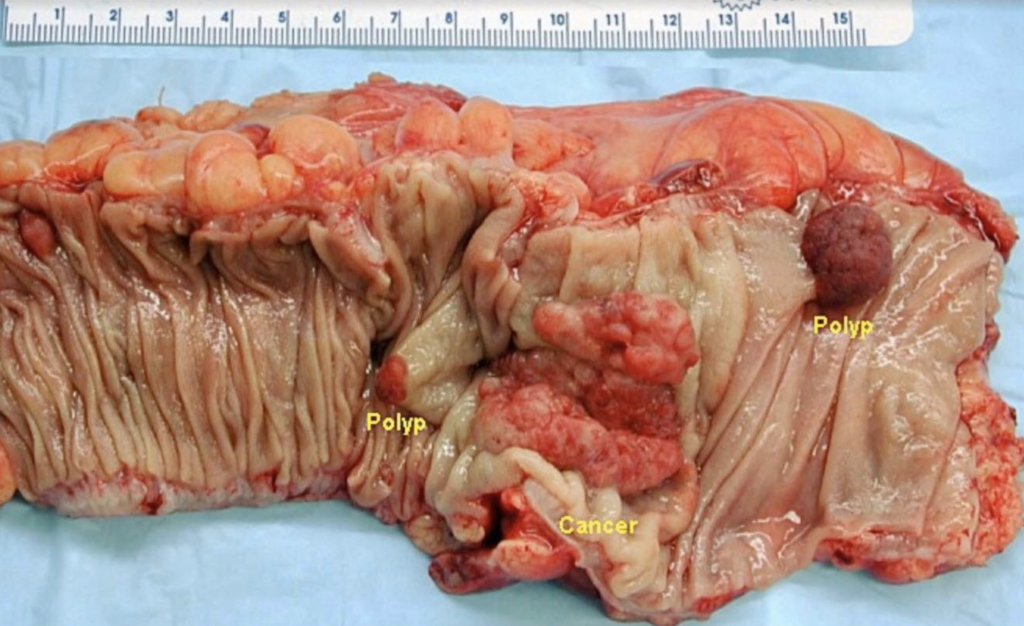
Most CRCs start as a growth on the inner lining of the colon or rectum. These growths are called polyps. Just bear in mind, though: Not all polyps become cancerous, but “a polyp has a potential for malignancy, and therefore it should be removed,” Dr. Dillera said. The procedure for the removal of polyps is called a polypectomy.
“If cancer forms in a polyp, it can grow into the wall of the colon or rectum over time,” the ACS states. “The wall of the colon and rectum is made up of many layers. CRC starts in the innermost layer and can grow outward through some or all of the other layers.
“When cancer cells are in the wall, they can then grow into blood vessels or lymph vessels (tiny channels that carry away waste and fluid). From there, they can travel to nearby lymph nodes or to distant parts of the body.”
No one knows what causes CRC. “Epidemiologic, human case-control, and animal studies support a strong association between colon cancer and a diet that has high-fat (usually saturated fat), low fiber, and high red meat consumption,” said Dr. Jun Ruiz, a diplomate of the American Board of Internal Medicine in Gastroenterology and of the Philippine College of Physicians in Internal Medicine.
Risk factors that predispose a person to develop colon and rectal cancer include age, personal history of adenoma or carcinoma, family history of CRC, and pre-existing diseases, like inflammatory bowel disease.
“Age 50 is the most common risk factor for CRC as 90% of cancers occur after the age of 50,” said Dr. Ruiz. As the Department of Health (DOH) puts it: “Colon cancer increases markedly after age 50.”
But with more recent information showing a rise in colon cancer among younger patients, “earlier screening should be performed,” said Dr. Dr. Laya-Zinampan. “Even earlier screening is encouraged when a family history of colon cancer is present.”
Several lifestyle-related factors have been linked to colorectal cancer. These include smoking, obesity, lack of physical activity, and alcohol intake.
In the past, CRC has been referred to as “a disease of the rich.” But such is not the case anymore. “(CRC) is more common in richer countries, but its incidence is rising in some developing countries,” the Geneva-based World Health Organization (WHO) reports. “The risk of developing those cancers that are typical of higher socioeconomic groups – cancers of the breast, colon, and rectum – can be expected to increase with economic development.”
CRC tends to grow slowly and may be asymptomatic for years, according to Dr. Ruiz. “Afflicted persons often have occult blood loss from their tumors, before they complain of symptoms. They can present with rectal bleeding and anemia, leading to fatigue, shortness of breath, and weight loss,” he says.
Dr. Ruiz says cancers of the right colon tend to grow larger than those of the left colon before symptoms occur. “Obstructive symptoms, like colicky abdominal pain, vague abdominal discomfort, change in bowel habits or stool caliber, and constipation, are found in advanced cases,” he adds.
Early detection of the dreaded disease can be achieved by screening tests. “CRC screening has resulted in reduction of related mortality up to 60-70%,” Dr. Ruiz says. “All methods have been proven to be cost-effective.”
Colonoscopy is the gold standard for CRC screening as it can detect and remove pre-cancerous polyps. “The procedure involves a flexible fiber-optic scope with a camera that is inserted through the rectum and is carefully advanced to visualize the colon under mild anesthesia,” explains Dr. Ruiz.
The anesthesia takes time to wear off completely after a colonoscopy. The patient may stay at the hospital or outpatient center for one to two hours after the procedure. Don’t be alarmed if you feel cramping in your abdomen or bloating during the first hour after the procedure.
Colonoscopy, which typically takes about 30 to 45 minutes, can cost between P15,000 to P30,000, depending on the hospital.
Some patients may not want to have an invasive test. A stool test called FIT is a good screening alternative and is not expensive (it costs less than P500). “(FIT) detects only human blood and is specific for bleeding in the colon,” Dr. Ruiz states. “The test is repeated every year if the initial test is negative. If the test is positive, a colonoscopy is needed to rule out the presence of cancer.”
In a press statement issued by Philippine Health Insurance Corporation (PhilHealth), expenses for the treatment and management of colon and rectum cancers are now covered for members who pass the selections criteria through the Z Benefit Package.
The package rate for the entire course of treatment of colon cancer for low risk is P150,000, while package rate for high risk is P300,000. For rectum cancer, the entire course of treatment for stage 1 (clinical and pathologic) is P150,000.
As a gastroenterologist who advocates colorectal cancer screening, Dr. Ruiz recommends a screening colonoscopy in individuals between 50 to 75 years of age who are relatively healthy and wherein the benefits of a colonoscopy outweigh the risks associated with the procedure.
“The patient has to understand that it requires a rigorous bowel preparation, and has more risks compared to the other alternative,” he explained. “The FIT is recommended to patients who may be at high risk for complications of a colonoscopy, or not willing to undergo a colonoscopy yet because of a variety of reasons.”
Colon cancer is deadly – but beatable if only it is discovered early. “The key here is screening patients who are already at risk for colon cancer,” Dr. Ruiz points out. “Patients may already have early cancer, even if they have no symptoms. We can also reduce the risk of colon cancer by removing pre-cancerous lesions (polyps) during a colonoscopy. In the end, CRC screening can just save your life or the life of a loved one.”
In addition to screening, “maintaining a healthy lifestyle is strongly encouraged,” Dr. Laya-Zinampan suggested. “High-fiber fruits and vegetables and whole grain should be included in the daily diet. Exercise to maintain a healthy weight and avoiding tobacco and alcohol are other ways to prevent colon cancer.”